RARE PRESENTATION OF A COMMON DISEASE
Hello everyone.....I am a 4th year MBBS student.Ihave been given this case to solve in an attempt to understand the topic of paraparesis.
Here is the link for detailed history and investigations of the patient;
PROBLEMS OF THE PATIENT IN ORDER OF PRIORITY:
- Bilateral lower limb weakness since 5 days
- Tingling and numbness
- Gluteal abscess operated 5 months back
- Scrotal abscess since 20 days(incicion and drainage done 10 days back)
PAST HISTORY:
History of multiple sexual partners.
No associated comorbidities.
KEY EXAMINATION FINDINGS:
HMF-normal
Speech-normal
Cranial nerves intact
MOTOR SYSTEM:
| RIGHT | LEFT | |
| BULK: | normal | normal |
| TONE:UL | normal | normal |
| LL | hypotonia | hypotonia |
| POWER:UL | 5/5 | 5/5 |
| LL | 2/5 | 0/5 |
| SUPERFICIAL REFLEXES: Corneal | present | present |
| Conjunctival | present | present |
| Abdominal | present | present |
| Plantar | extensor | extensor |
| DEEP TENDON REFLEXES: Biceps | 2+ | 1+ |
| Triceps | 2+ | 1+ |
| Supinator | 3+ | 2+ |
| Knee | 3+ | 2+ |
| Ankle | 3+ | 2+ |
| Jaw jerk | 1+ | 1+ |
| Ankle clonus | present | absent |
Primitive reflexes:absent
Involuntary reflexes:absent
SENSORY SYSTEM:NORMAL
CEREBELLUM:NORMAL
NO MENINGEAL SIGNS
ANATOMICAL LOCAIZATION OF SITE OF LESION:
- BILATERAL HYPOTONIA:feature of LMN lesion
- KNEE AND ANKLE HYPERREFLEXIA:feature of UMN lesion
- Ankle clonus and extensor plantar response:features of UMN lesion
Hypertonia and hyperreflexia are features of UMN lesion(pyramidal insufficiency) due to loss of descending inhibition from the upper motor neurons.
However there may be a acute presentation of hypotonia and hyporeflexia after UMN injury.This is called SPINAL SHOCK.This represents disturbed spinal circuits after sudden deprivation of input from motor cortex.
LMN findings are not uncommon after a UMN injury.These are seen in acute brain and spinal cord insults.
I would like to share this article which explains the possible theory behind acute LMN findings after a UMN lesion:
MRI and X-RAY findings of the patient revealed significant enhancing lesions in right and left cerebral hemispheres and multiple nodules in pulmonary apices suggestive of pulmonary kochs and disseminated tuberculosis.
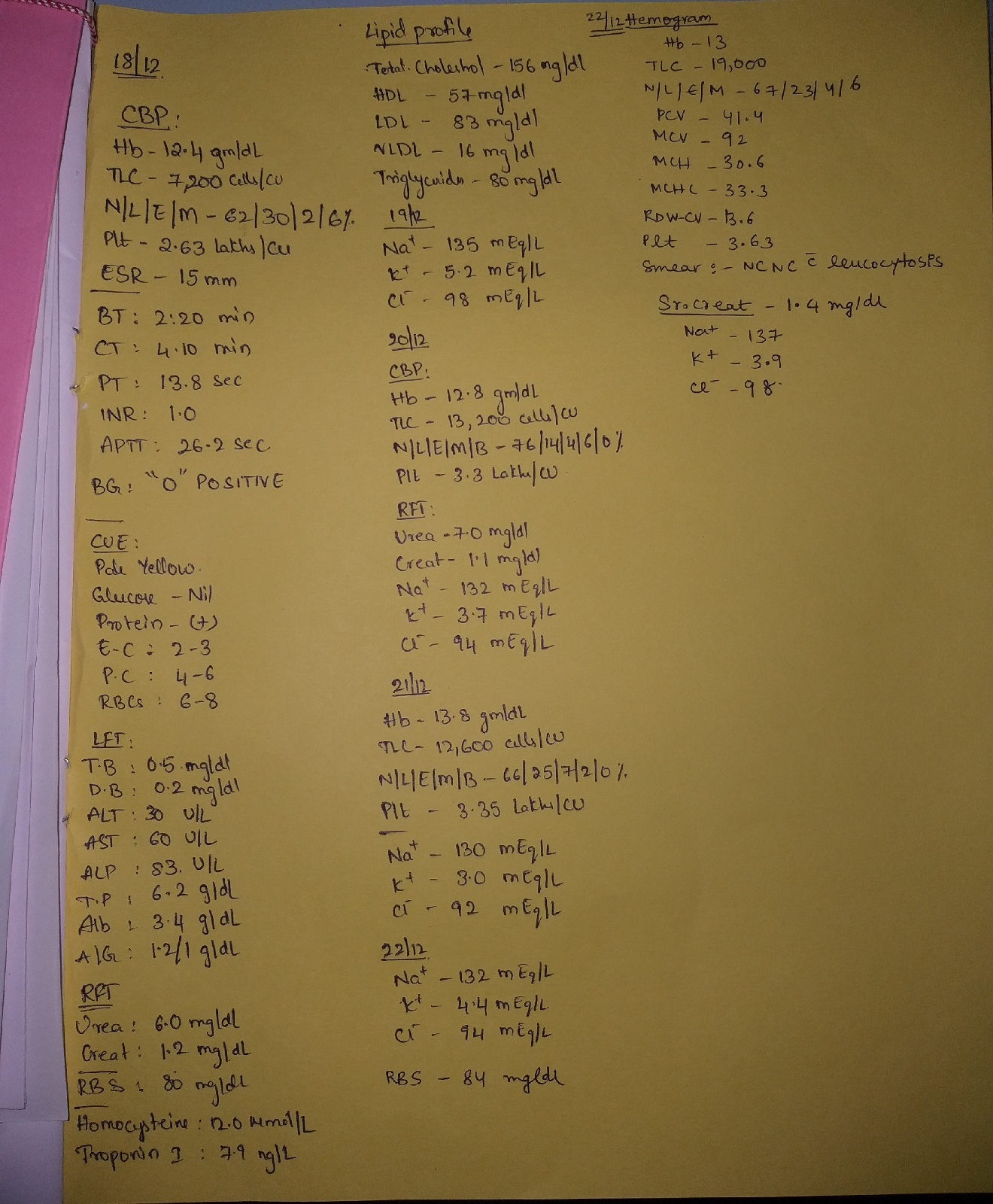
KEY INVESTIGATION FINDINGS:
- HBsAg: negative,AntiHCV ABs:non reactive,HIV: nonreactive.
- LFT:
Total bilirubin-0.82 mg/dl
Direct bilirubin-0.21mg/dl
SGOT-80 IU/L
SGPT-10 IU/L
ALP-192 IU/L
Total protein-7.5 gm/dl
Albumin-4 gm/dl
A/G ratio-1.19
- ESR:45mm/1st hr
Tuberculosis is a chronic inflammatory condition which causes increase in levels of acute phase reactants causing rise in the ESR value.
DIFFERENTIAL DIAGNOSIS:
- Bilateral Anterior cerebral artery vasculitis secondary to disseminated TB
- L4,L5 Spondylodiscitis
- Pott's paraplegia
PATHOLOGICAL DIAGNOSIS:
- Bilateral ACA vasculitis
Mycobacterium tuberculosis may invade the vessel wall directly or there may be deposition of immune complexes leading to occlusion of vessels and infarction.
Ring enhancing lesions on MRI suggest tubercular granulomas.
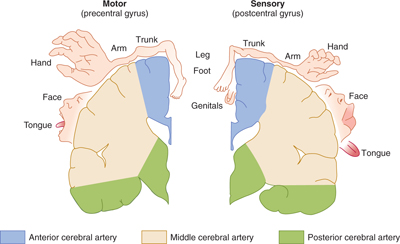
The two anterior cerebral arteries arise from internal carotid artery and are a part of the circle of willis.Anterior cerbral artery supplies the most midline portions of frontal and superior medial parietal lobes.
The leg areas in the cortical motor homunculus are represented in the medial surface of hemispheres.
Tb bacilli thus might have spread via bloodstream and caused bilateral ACA infarcts resuting in paraparesis.
2.L4,L5 Spondylodiscitis
It is commonly seen in immunocompromised individuals.Inflammation of adjacent vertebrae and the corresponding intervertebral disc is also commonly caused by mycobacterium tuberculosis.
The psoas abscess in this patient could be secondary to vertebral infection.
3.Pott's paraplegia
TB of spine mainly involves dorsolumbar vertebrae.Pott's spine can cause spinal cord compression and paralysis below the level of compression.
There are definite features of pott's spine in this case.
FURTHER INVESTIGATIONS:
- Sputum examination
- Mantoux test
- Aspiration of psoas abscess and culture and sensitivity of the fluid.
SUGGESTED TREATMENT:
- Antitubercular therapy
- T.Benadon 40mg/od
- T.Pregabalin 75mg/po/h/s
- OINT.MEGAHEAL
- SITZ BATH with betadine tid
- Frequent change of position
My references:

Comments
Post a Comment