MEDICINE ONLINE ASSESSMENT
A case of 45 year old lady with history of pedal edema which got progressed into abdominal distension and facial puffiness associated with decreased urine output,shortness of breath and chest pain on right side non radiating with intermittent palpitations.
Link to the above case:
https://alekyatummala.blogspot.com/2020/09/45-yr-female-with-anasarca.html?m=1
1)What is the complete anatomic and etiologic diagnosis from data available in patient's online record linked above?
ANATOMIC DIAGNOSIS:
Chronic kidney disease
ETIOLOGIC DIAGNOSIS:
Diabetic nephropathy
The disease progression in diabetic nephropathy involves various clinical stages:hyperfiltration,microalbuminuria ,macroalbuminuria,nephrotic proteinuria to progressive CKD leading to end stage renal disease.The damage is seen in all compartments of kidney:glomerulus,renal tubules,vasculature and interstitium.Renal fibrosis is the final common pathway of diabetic nephropathy.
Initially there is constriction of efferent arterioles and dilation of afferent arterioles with resulting glomerular hyperfiltration and glomerular capillary hypertension this gradually changes to hypofiltartion over time.Changes in the glomerulus include basement membrane thickening,widening of slit membranes of podocytes,increase in mesangial cells and matrix.This matrix invades capillaries and produces deposits called kimmelsteil wilson nodules,the cells and matrix completely expand and consume entire glomerulus shutting off the filtration.
https://en.wikipedia.org/wiki/Diabetic_nephropathy

https://www.grepmed.com/images/3123/pathophysiology-nephropathy-nephrology-diabetic-ckd
The other risk factors of CKD in this patient are hypertension and drugs she is used (query about use of NSAIDs,ACE inhibitors/ARBs should be made).
2)What are the reasons for her:
AZOTEMIA:Azotemia is an elevation of blood urea nitrogen and serum creatinine levels.Normally urea is reabsorbed from the tubules but creatinine is not reabsorbed therefore it approximately equals GFR.
Intrinsic/Intrarenal azotemia results from damage to kidney itself(glomeruli,tubules,interstitium and vasculature).This may result from vasculitis,toxins,drugs,infections and damage from hypoperfusion.
- BUN:creatinine ration<20:1
- FeNa>2
- Urine osmolality<300 mOsm/kg
- Urine analysis:cellular debris,muddy brown red cell casts and eosinophils may be seen,proteinuria is present.
- Deficiency of erythropoeitin
- Toxic effects of uremia on bone marrow precursor cells
- Blood loss due to capillary fragility and poor platelet function
- Reduced intake,absorption and utilisation of dietary iron
- Anemia of chronic disease
- Proteinuria
- Malnutrition
- Inflammatory status in poorly controlled diabetes mellitus
- Metabolic acidosis
 https://link.springer.com/chapter/10.1007/978-1-84800-334-7_10
https://link.springer.com/chapter/10.1007/978-1-84800-334-7_10
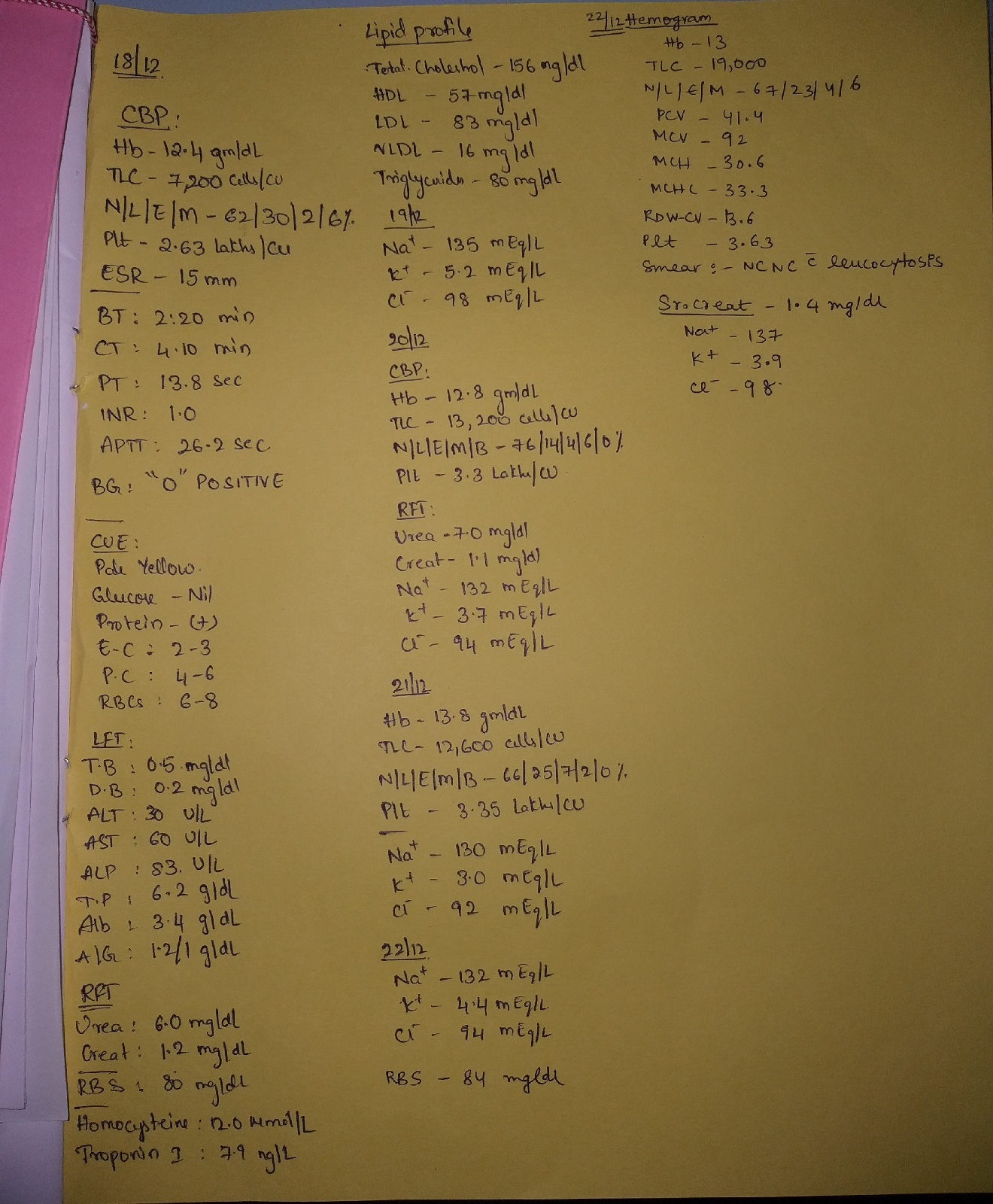
3)What was the rationale for her treatment plan detailed day wise in the record?Particularly mention rationale and efficacy for some drugs such as oral and iv bicarbonate?When is iv or oral bicarbonate indicated and why is contraindicated in certain situations?
- Inj.NaHCO3 is used to treat metabolic acidosis and to reduce tubulointerstistial inflammation.For mild acidosis usual dosage is 1 to 2 mEq/kg body weight administered slowly.For more severe acidosis 2 to 5 mEq/kg body weight may be used.Overdose may result in severe degree of alkalosis which may be treated by calcium gluconate or an acidifying agent.
- NaHCO3 is contraindicated in patients with hypocalcemia in which alkolosis may produce tetany.It is also contraindicted in excessive chloride loss and hypokalemia.
- Injection insulin according to sliding scale:How much insulin needs to be given to patient is decided based on her blood glucose levels.
- Inj.lasix is a loop diuretic for the treatment of oedema.
- Tab.orofer xt and Inj.erythropoeitin to treat the anemia.
- Oral syp.potchlor 15ml=20 mEq to treat mild-moderate hypokalemiaTreatment of acidosis with NaHCO3 may aggravate or precipitate hypokalemia due to intracellular shift of K+.Never give injection direct iv it can cause sudden hyperkalemia and instant death from cardiac arrest.
- Tab.telma and nicardia to treat her hypertension.
- Tab.shelcal for correction of secondary hyperparathyroidism.
- Severe metabolic acidosis and refractory anuria.
- Possible exposure to certain drugs like NSAIDs.
- Malnutrition and iron deficiency anemia.
- Older age.

https://www.ahajournals.org/doi/full/10.1161/circulationaha.116.022249
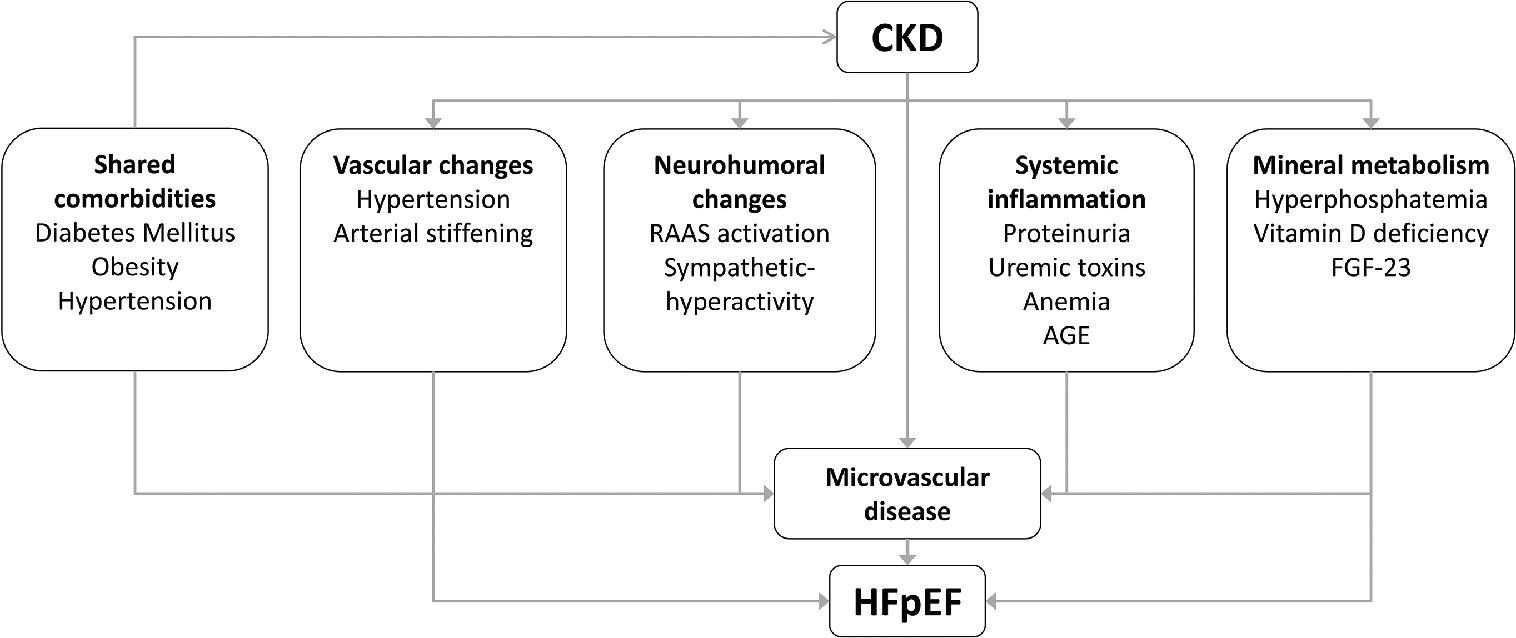
https://www.frontiersin.org/articles/10.3389/fphys.2019.01108/full
Diagnosis of cardiorenal HFpEF:
- Biomarkers for myocardial injury(troponin) and wall tension(BNP/NT-proBNP)
- Echocardiography
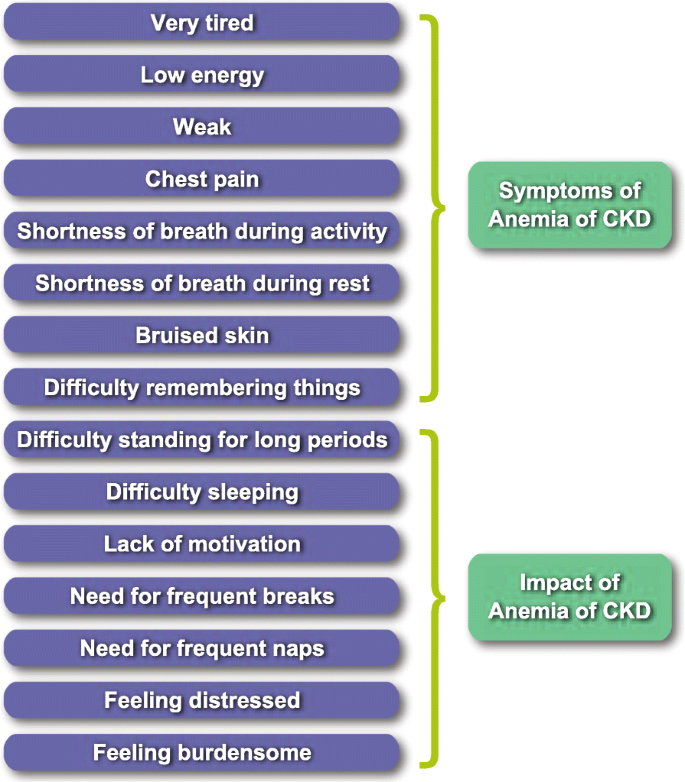 mptoms and impacts of anemia in CKD.
mptoms and impacts of anemia in CKD.https://link.springer.com/article/10.1186/s41687-020-00215-8
The CKD-AQ went through linguistic validation into 71 languages ,30 of which were asia -pacific languages.
https://www.valueinhealthjournal.com/article/S1098-3015(18)35623-7/fulltext
10)What is the contribution of protein energy malnutrition to her severe hypoalbuminemia?What is the utility of tools such as SGA subjective global assessment in evaluation of malnutrition in CRF patients?
Nutritional assessment of patients in CKD is of vital importance.SGA is tool that uses 5 components of medical history (weight change,dietary intake,gastrointestinal symptoms,functional capacity,disease and its relation to nutritional requirements)and 3 componentsof brief physical examination (signs of fat and muscle wasting,nutrition-associated alternations in fluid balance) to assess nutritional status.
Comments
Post a Comment