18 YEAR OLD PARAPARESIS CASE-2
Hello everyone.....I am a 4th year MBBS student.I have been given this case to solve in an attempt to understand the topic of paraparesis.
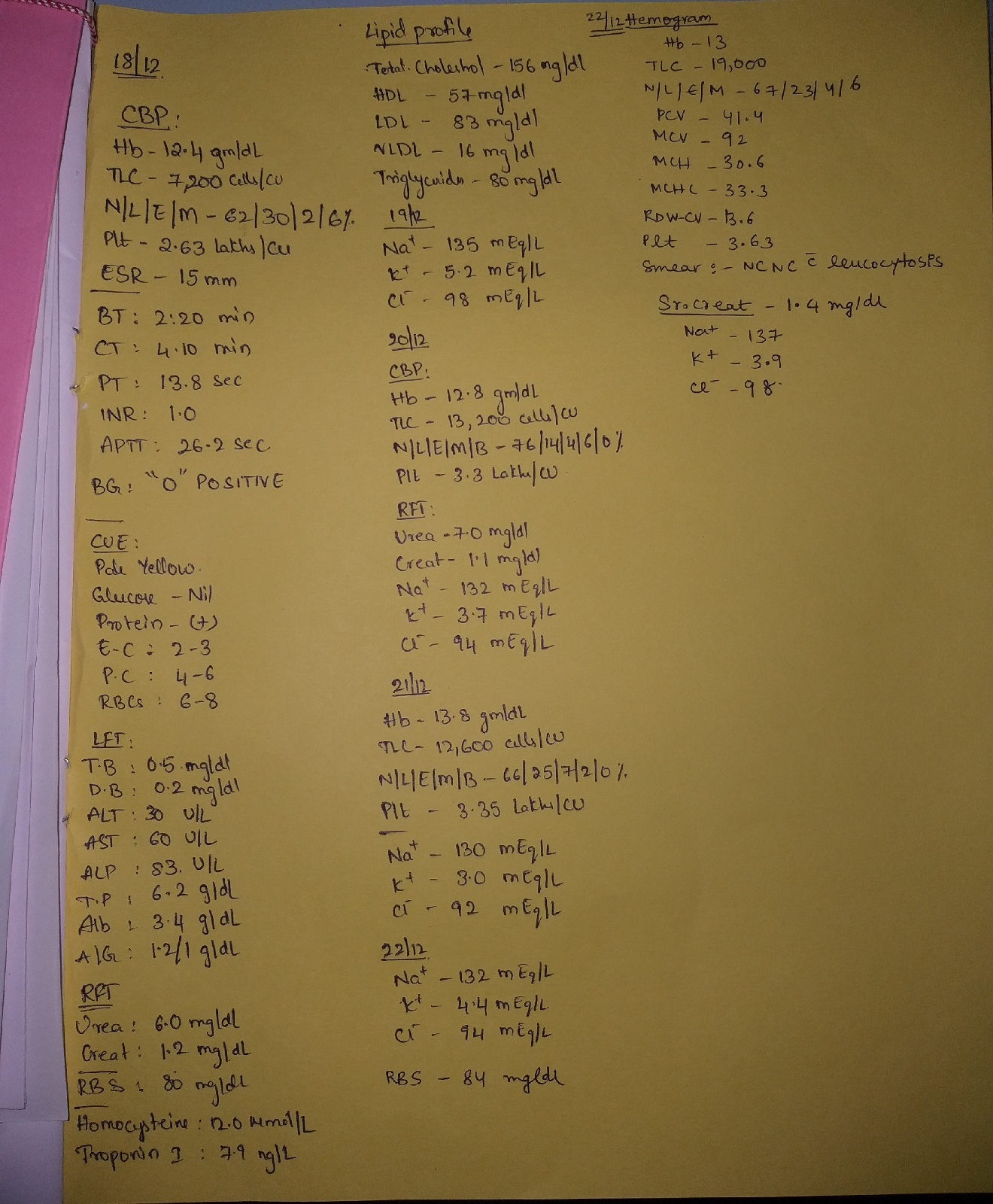
Here is the detailed history and investigations of the patient:
BRIEF HISTORY OF THE PATIENT AND HIS PROBLEMS IN ORDER OF PRIORITY:
18 year old male presented with:
- Bilateral lower limb weakness since 1 month.Weakness in proximal and distal muscles.
- History of wasting and thinning of muscles.
- History of pain in the calf muscles while walking.
Weakness may be due to upper motor or lower motor neuron diseases.
PAST HISTORY:
Not a known case of DM/HTN/Epilepsy/CVA/CAD.
PERSONAL HISTORY:
Diet:mixed
Appetite:normal
Bowel and bladder movements:regular
History of alcohol consumption since 2 years:twice weekly
No history of smoking
FAMILY HISTORY:
No significant history.
NERVOUS SYSTEM EXAMINATION:
Higher mental functions-normal
Cranial nerves-intact
MOTOR SYSTEM:
| RIGHT | LEFT | |
| BULK | decreased | decreased |
| TONE:UL | normal | normal |
| LL | hypotonia | hypotonia |
| POWER:UL | 4/5 | 4/5 |
| LL | 3/5 | 3/5 |
| Deep tendon reflexes: | ||
| Biceps | present | absent |
| Triceps | absent | absent |
| Supinator | absent | absent |
| Knee | absent | absent |
| Ankle | absent | absent |
SENSORY SYSTEM:normal
CEREBELLUM:normal
ANATOMICAL LOCALIZATION OF SITE OF LESION:
No upper motor neuron lesion signs are seen like spasticity,clonus,hyperreflexia,hypertonia and extensor plantar response.Therefore UMN lesion can be ruled out.
Hypotonia,absent deep tendon reflexes,muscle wasting suggest a lower motor neuron lesion.
SITES OF LOWER MOTOR NEURON LESION:
- ANTERIOR HORN CELL
- SPINAL NERVE ROOT AND PLEXUS
- PERIPHERAL NERVE
- NEUROMUSCULAR JUNCTION
- MUSCLE
AHC lesions,radiculopathies and plexopathies often present asymmetrically.
NMJ problems show typical fatiguability,fluctuating weakness and ocular/pharyngeal musle involvement.
Myopathies are pure motor lesions,they also have a symmetrical muscle invovement but reflexes are intact.
Thus it is clear that the lesion is in the peripheral nerves.
ETIOLOGICAL DIAGNOSIS:
Peripheral polyneuropathies can be axonal or demyelinating.
Nerve conduction studies help in identifying the type of neuropathy.
| AXONAL | DEMYELINATING | |
| MOTOR NCS: CMAP | decreased | normal |
| Distal latency | normal | prolonged |
| Conduction velocity | normal | slow |
| Conduction blocks | absent | present |
| F wave and H reflex | normal/absent | prolonged/absent |
NCS of the patient revealed bilateral common peroneal and sural axonal neuropathy.
CAUSES OF AXONAL NEUROPATHY:
- Alcoholism
- Diabetes mellitus
- Hypothyroidism
- Vitamin deficiencies(B1,B12,E)
- Drugs(isoniazid,pyridoxine,phenytoinchloroquine,certain anticancer drugs)
- Hereditary motor sensory neuropathy(CMTD type 2)
KEY INVESTIGATION FINDINGS:
- Perpheral blood smear was normal:no evidence of megaloblastic anemia(VIT-B12 deficiency)
- Thyroid profile:T3 levels-mild decrease,TSH-normal
- HIV serology:negative
Chronic alcohol consumption causes painful peripheral neuropathy.Associated nutritional deficiencies and direct toxic effect of alcohol results in alcoholic neuropathy.
PATHOPHYSIOLOGY OF ALCOHOLIC POLYNEUROPATHY:
- Acetaldehyde is toxic to peripheral nerves.
- Thiamine deficiency is common in chronic alcoholics.Cells cannot maintain the levels of ATP in the absence of thiamine.
Effects of alcohol depend on:frequency of drinking,quantity consumed,age of onset of drinking,duration of drinking,gender and genetic factors.
FURTHER INVESTIGATIONS:
- Sural nerve biopsy is planned
TREATMENT OPTIONS:
- VITAMIN B COMPLEX SUPPLEMENTATION
- Physiotherapy
- Management of calf pain
My references:

Comments
Post a Comment